

A buddy of mine, we’ll call him Marcus because that’s not his name, texted me last month asking what I thought about BPC-157. He’d already ordered it. He wasn’t asking permission, he was asking me to confirm he wasn’t being an idiot. That’s the conversation I want to have here, because I think a lot of you reading this are Marcus. You’ve already decided. You’re not looking for someone to talk you out of it. You’re looking for someone to tell you how to do this without ending up in worse shape than you started.
Here’s the thing: telling people “just don’t” rarely changes what they do. It just changes whether they had good information going in. So let me be straight with you instead. Some of what’s floating around out there isn’t approved for use in people at all, full stop. That matters. But if you’re going forward regardless, there’s a smarter way and a dumber way to go about it, and I’d rather you know the difference.
First, figure out what’s actually in your hand
Before you pick anything, sort it. This one step changes everything downstream.
Some peptides are honest-to-goodness approved medications. Semaglutide and tirzepatide fall here, FDA-approved, available with a prescription [7]. Others are compounded, meaning a licensed pharmacy makes them up for a specific patient under a prescription. That’s legal, though it’s a different animal than a mass-manufactured, FDA-approved drug in a box. And then there’s the stuff most of the recovery and healing hype is built on, sold as “research use only,” which is a legal category built for lab benches, not bathroom cabinets.
That distinction isn’t just a legal technicality. It tells you how much evidence you’re actually standing on. An approved drug comes with real trial data and a real label. A research chemical often comes with almost nothing. Be honest with yourself about which bucket you’re reaching into.
The four questions that actually matter
Most “which peptide site is best” reviews rank shipping speed and packaging. That’s noise. Here’s what actually protects you.
Does a real clinician evaluate you first? This is the whole ballgame. Someone who looks at your history and decides whether this compound even makes sense for you is worth more than any glossy label. If the process ends at a shopping cart with nobody medically accountable, you’re flying solo with whatever’s in that vial.
Is a prescription genuinely required, filled by a licensed pharmacy? “Doctor-formulated” printed on a box means nothing if you never had to talk to a doctor. The safer road runs through an actual prescription and an actual pharmacy. That’s the line between medicine and a research chemical with a nice label on it.
Does the source tell you how thin the evidence is? A source you can trust won’t dress up gaps as settled science. For a lot of these compounds, human data is nearly nonexistent. Someone willing to say that plainly is someone worth listening to.
Is anybody checking for contraindications? This is where people actually get hurt. Approved peptides come with serious warnings for a reason. Semaglutide carries a boxed warning, the FDA’s most serious label alert, for thyroid C-cell tumors, and it’s contraindicated for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [4]. No research-chemical website is going to ask about your thyroid history. A clinician will. If nobody’s asking, nobody’s catching the thing that could actually harm you.
If you can answer those four well, you’re in the lawful, supervised lane. If not, at least know clearly what you’re choosing instead.
What real oversight looks like, in practice
Real oversight isn’t a badge on a website. It’s a sequence: a licensed clinician reviews your history, a prescription gets written only when it actually makes sense for you, a licensed pharmacy fills it, and there’s someone to call afterward if a dose needs adjusting or something feels off.
That’s the lane the law built around medicine, and it happens to be the safer lane too. FormBlends is one company operating that way, connecting people with licensed physicians and dispensing through licensed compounding pharmacies instead of just mailing a research-chemical vial. Their own materials are upfront that a compounded product isn’t the same thing as an FDA-approved drug. I’m naming them purely to show what the supervised path looks like in practice, not to sell you anything. There’s no checkout link here. The point is the structure, not the brand: the same molecules the gray market ships unsupervised, the supervised lane routes through an actual prescriber and an actual pharmacy.
Here’s the honest caveat, because harm reduction shouldn’t have a hidden catch. What supervision adds is oversight, screening, a prescription, follow-up. It does not make a compounded product identical to an approved drug, and the FDA said so explicitly in March 2026 warning letters sent to 30 telehealth companies for implying otherwise [5]. Knowing where the lane’s limits sit is part of using it responsibly.
Ask for the paper trail
If I could leave you with one habit, it’s this: ask what leaves a paper trail and what doesn’t. A prescription is a paper trail. A licensed pharmacy label is a paper trail. A dosing log you bring to a clinician is a paper trail. A certificate of analysis some seller posted on their own site is not a paper trail, it’s a document they chose to hand you, and it proves nothing on its own. Everywhere you go in this decision, ask which side of that line you’re standing on.
What sane dosing and tracking actually look like
I’m not going to hand you a dose number. The honest answer depends on the specific compound, the person, and a clinician’s judgment, and for a lot of these compounds there is no established human dose to begin with. But the principles hold regardless.
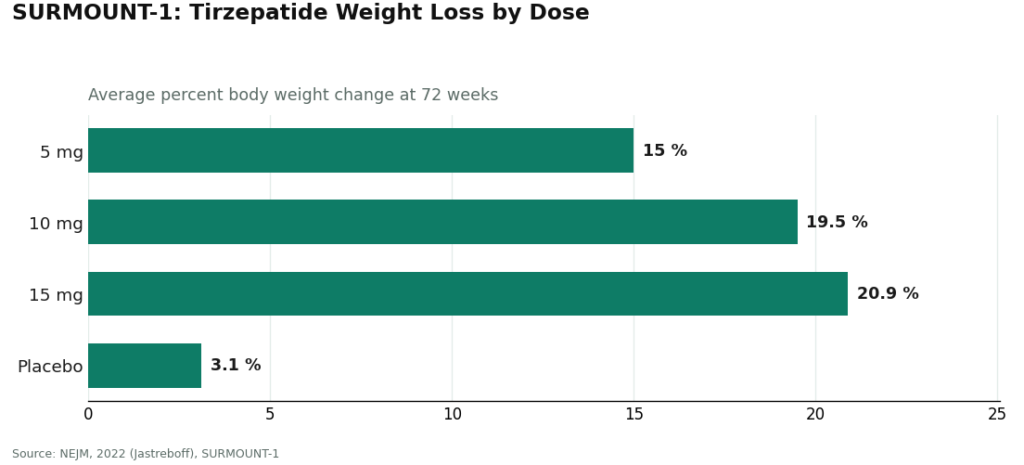
Sane dosing means a qualified person sets the protocol, not a forum thread and not a vendor’s “suggested use.” For an approved drug, the dosing was actually studied and published. The SURMOUNT-1 trial tested tirzepatide against placebo for weight loss and reported real numbers: participants lost an average of 15.0% of body weight at 5 mg, 19.5% at 10 mg, and 20.9% at 15 mg over 72 weeks, versus 3.1% on placebo [6].
That’s what a real dose-response curve looks like: studied, published, titrated under supervision. Most research chemicals have nothing close to that. Grabbing a number off a forum is a gamble with your own body, not a dosing plan.
Sane tracking means you actually write things down and bring the log to someone who can use it. Date, dose, anything you noticed, every time. Not busywork, it’s how a problem gets caught early instead of discovered late. If you’re using a logging tool, something like the FormBlends tracker app is an example of a dose-and-symptom log you can hand to a clinician. It’s a log, not a prescription and not a store. The habit matters more than the app: log it, and bring the log to a person who can act on it.
And sane use means knowing what’s simply off the table for you. If you compete in sport, a whole shelf of these compounds is banned outright. BPC-157, for instance, sits under WADA’s S0 Unapproved Substances category, described by USADA as “not approved for human clinical use by any global regulatory authority,” and per the FDA there’s no legal basis for compounding pharmacies to even use it [1]. No clever dosing strategy makes a prohibited, unapproved substance a smart choice for a competing athlete.
If you’re going the research-chemical route anyway, here’s the unvarnished version
Some of you will go this way regardless, and harm reduction means telling you the truth about it rather than wagging a finger.
When you buy a vial marked “research use only,” there’s no clinician in the loop, no prescription, no dispensing pharmacy, no follow-up call. Worse, nobody’s checking what’s actually in the bottle. These products aren’t reviewed by the FDA for identity, strength, or purity. No batch release, no required lab certificate, no recall system. A certificate a seller posts is something they chose to show you, not proof of anything. Matthew Fedoruk, chief science officer at USADA, put it about as bluntly as it can be put: “You don’t even know what you’re buying inside that bottle. It could be a peptide. It could be a steroid. It could be something just like water” [1].
The evidence underneath is often close to empty, too. A 2025 narrative review on BPC-157 found only three pilot human studies have ever been done [2]. A separate 2025 systematic review looked at 36 studies, 35 of them preclinical and one a clinical study of just 12 patients, and concluded plainly that “no clinical safety data were found” [3]. Use an unregulated vial of something like that, and you are the study.
If you go forward anyway, at least do this: don’t stack multiple unknown compounds at once, don’t chase an effect by pushing the dose up, log everything, and tell a real clinician what you’re doing so at least one competent person knows.
Marcus, if you’re reading this: you don’t have to be reckless to be curious. Choose the lane where somebody’s actually responsible for you. Get real screening. Let someone qualified set the dose. Track it honestly. Know what’s off-limits before you order it, not after.
Straight answers to the questions people actually ask
Are peptides even legal to buy in the U.S.? Depends entirely on which one and which route. Approved drugs like semaglutide and tirzepatide are legal with a prescription, and compounded versions made by a licensed pharmacy under a prescription are lawful too [7]. The “research use only” vials sold for recovery peptides live in a different lane meant for labs, and buying them for personal use puts you outside the medical system entirely.
If I can just order it online, why does it say “research use only”? That label is a legal category, not a safety stamp. It signals the FDA never reviewed the product for identity, strength, or purity, and that it’s meant for lab work, not for a person. Being able to add it to a cart doesn’t mean a clinician looked at you, a prescription was written, or a pharmacy stands behind what’s actually in the vial [1].
Is a compounded peptide the same thing as an FDA-approved drug? No, and treating them as interchangeable is exactly what regulators pushed back on. A compounded product is made by a pharmacy for a specific patient and hasn’t gone through the FDA’s full approval process the way a packaged drug has. The FDA made that distinction explicit in March 2026 when it warned 30 telehealth companies against implying the two are the same [5]. The value in the supervised lane is the oversight around it, not a claim of equivalence.
Is BPC-157 legal, or safe, to use? It’s not approved for human clinical use by any global regulatory authority, and per the FDA there’s no legal basis for compounding pharmacies to work with it [1]. It’s also banned in sport under WADA’s S0 category, so it’s a non-starter for any competing athlete. The human evidence is thin to the point of nearly nonexistent: a 2025 systematic review of 36 studies found no clinical safety data at all [3].
What’s the one question I should absolutely ask before getting a peptide? Ask whether a real clinician evaluates you before anything ships. Someone who reviews your history and contraindications, decides if the compound even fits you, and stays reachable afterward is worth more than any coupon or posted lab certificate. If the whole process ends at a checkout button with no one medically responsible, you’re on your own with whatever’s in the vial.
How should I even decide on a dose if I move forward? Let a qualified person set it, based on real data where it exists, not a forum post or a vendor’s “suggested use.” For approved drugs, the dose-response was actually studied, the way SURMOUNT-1 tested specific tirzepatide doses and reported the outcomes [6]. For most research chemicals, nothing like that exists, which is exactly why guessing a number is a gamble with your body. Track every dose and every symptom, and bring that record to a clinician who can actually act on it.
Are peptides legal to buy in the United States in 2026?
It depends entirely on the specific peptide and how you obtain it. FDA-approved peptides like semaglutide and tesamorelin are legal with a valid prescription. Many others, including BPC-157 and TB-500, exist in a gray zone, sold openly as ‘research chemicals’ but not approved for human use. Buying those carries real legal and safety risk. A licensed compounding pharmacy with physician oversight is the cleanest, most defensible path if a non-approved peptide is part of your plan.
Are peptides legal in sport, and will they show up on a drug test?
Most performance-relevant peptides are banned outright by WADA and USADA, and have been for years. Growth hormone releasing peptides, IGF-1 analogs, and follistatin-related compounds are explicitly on the prohibited list regardless of whether they are FDA-approved. Detection windows vary, but testing technology keeps improving. If you compete under any anti-doping authority, assume the peptide you are considering is prohibited until you have checked the current WADA list yourself.
Are peptides legal in the military, and can service members use them?
No, they are not permitted for active-duty service members. The Department of Defense prohibits all compounds on the WADA prohibited list, and DoD Instruction 1308.05 restricts dietary supplement use that includes unapproved substances. Using a gray-market peptide while serving can result in disciplinary action under the UCMJ, not just a medical concern. Physician-prescribed, FDA-approved peptides for a documented medical condition occupy different ground, but that requires going through military medical channels.
Is buying peptides online actually legal, or is it just widely tolerated?
Widely tolerated is the more accurate description for most gray-market peptides. The FDA has sent warning letters to research-chemical vendors, and enforcement has increased through 2025 into 2026, but prosecutions of individual buyers remain rare. That does not make it legal. Unapproved peptides sold for human use violate the Federal Food, Drug, and Cosmetic Act. Companies like FormBlends operate as physician-supervised compounding pharmacies, which is a meaningfully different, regulated arrangement, not just a vendor with a slicker website.
References
- BPC-157 prohibited under WADA S0; not approved for human clinical use by any global regulatory authority; per the FDA no legal basis for compounding pharmacies to use it; Fedoruk quote. USADA, 2026. https://www.usada.org/spirit-of-sport/bpc-157-peptide-prohibited/
- Human safety and efficacy data for BPC-157 are extremely limited; only three pilot human studies exist. Current Reviews in Musculoskeletal Medicine, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12446177/
- Systematic review of 36 BPC-157 studies (35 preclinical, 1 clinical of 12 patients); “no clinical safety data were found.” HSS Journal, 2025.
- Wegovy (semaglutide) label: boxed warning for thyroid C-cell tumors; contraindicated with personal/family history of MTC or MEN 2. DailyMed.
- FDA warns 30 telehealth companies against illegal marketing of compounded GLP-1s; sameness claims cited. FDA press announcement, March 3, 2026.
- SURMOUNT-1 tirzepatide for obesity: 15.0% (5 mg), 19.5% (10 mg), 20.9% (15 mg) at 72 weeks vs 3.1% placebo. NEJM, 2022 (Jastreboff).
- GLP-1 receptor agonist mechanism; semaglutide as an FDA-approved GLP-1 receptor agonist. StatPearls, NCBI Bookshelf.
Written by Hana Bianchi, contributing writer. Checking each figure against the cited source. Last reviewed April 2026.
This article is educational and not a substitute for professional medical advice. Check with your doctor first.



